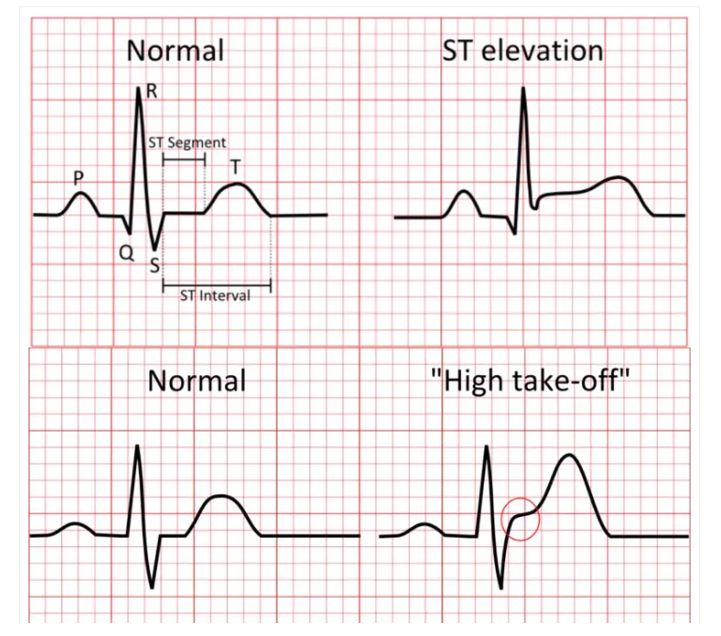
A STEMI, or ST-elevation myocardial infarction, is the most dangerous type of heart attack. It occurs when a coronary artery becomes completely blocked—usually after a cholesterol plaque ruptures and a clot rapidly forms—cutting off oxygen to a section of the heart muscle. On a 12-lead ECG, this appears as an abnormal upward lifting of the normally flat ST segment above the baseline, creating a shape some clinicians compare to a tombstone. This elevation is visible in contiguous leads that look at the same part of the heart (such as the inferior, anterior, or lateral walls), signaling full-thickness injury. The BMJ Best Practice guideline defines STEMI as new or increased, persistent ST-segment elevation in at least two contiguous leads of ≥1 mm in all leads other than V2–V3, where more specific age- and sex-based cutoffs apply: ≥2.5 mm in men under 40, ≥2 mm in men over 40, and ≥1.5 mm in women regardless of age.
Typical symptoms include crushing chest pain that may radiate to the jaw, arm, or back, along with shortness of breath, sweating, nausea, or lightheadedness. However, women, older adults, and people with diabetes often experience more subtle signs—what clinicians call anginal equivalents—such as dyspnea, fatigue, syncope, or persistent vomiting. Because "time is muscle," meaning every minute of delay causes more permanent heart damage, emergency treatment focuses on reopening the artery as fast as possible.